Elsewhere, I’ve discussed the potential of two
female-associated hormones, estrogen and
progesterone, to be neuroprotective after
spinal cord injury. Both inhibit a variety of neuron-damaging processes
that occur after SCI and, by so doing, may limit neuronal tissue loss
and preserve function. This installment will specifically provide an
overview of testosterone and testosterone replacement therapy (TRT).
Although viewed as the virilizing male hormone,
women also produce small amounts of testosterone. The hormone is
primarily produced by the testes in men and the ovaries and placenta in
women. Small amounts are also produced by the adrenal glands. In men,
testosterone promotes 1) the development of reproductive tissue, sex
organs, and secondary sexual characteristics such as body hair and voice
deepening (i.e., androgenic role); and 2) sexual function, growth of
muscle mass and strength, and bone density (i.e., anabolic influence).
The second benefit also makes testosterone important in women.
Testosterone Production
Testosterone is synthesized from cholesterol, which
is an essential biochemical building block for many hormones and
nervous-system molecules. Its production is regulated by the
hypothalamic-pituitary-testicular axis, a tongue-tying description for a
regulatory, feedback loop used by our bodies to attain hormonal balance.
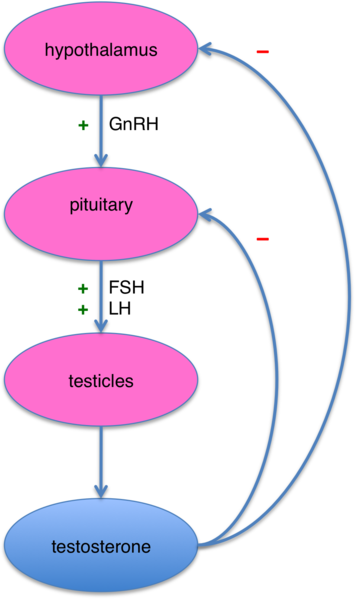
Briefly, the hypothalamus, a region of the brain
located above the brain stem, regulates the release of key hormones by
the nearby pituitary gland, which then stimulates testicular cells to
produce testosterone. However, as testicular production increases, the
elevated testosterone levels start shutting off the brain’s release of
testosterone-stimulating molecules. As a result, testosterone output
decreases (figure). Because testosterone synthesis is
central-nervous-system-driven process, a major CNS disruption like SCI
can affect testosterone levels.

Carried via the bloodstream, the
testicular-synthesized testosterone (or its derivatives) reaches the
target tissue, such as muscle, bone, sex organs, kidney, liver, and
brain. It is then transported into the cells and interacts with the DNA
of specific genes. This interaction cranks-up gene expression and, in
turn, the tissue products resulting from that expression - e.g., more
muscle, etc. As a simple analogy, it’s like speeding up a manufacturing
assembly line.
Testosterone Levels
Normal testosterone blood levels range from about
300-1,000 and 25-90 nanograms per deciliter in men and women,
respectively (nanogram is one-billionth of gram (~28 grams/ounce);
deciliter is one-tenth of liter).
Only about two percent of the body’s testosterone
is biologically active free testosterone. The remaining
testosterone is either 1) bound to albumin, a carrier protein in
the blood plasma (yet still bioavailable), or 2) complexed with sex
hormone binding globulin (SHBG) (no longer bioavailable). To give a
better idea of one’s true testosterone status, laboratory assessments
should measure both total and free testosterone.
Low testosterone levels are referred to as
hypogonadism, a condition associated with osteoporosis (loss of bone
density), decreased lean body mass (i.e., more fat), less strength,
reduced mental acuity and focus, mood changes, fatigue, less sexual
desire, and erectile dysfunction. As men age, testosterone levels
decline, a process called andropause after middle age.
In addition to age, various factors contribute to
low testosterone levels. For example, 1) excessive amounts of the
hormone can be converted into estrogen, 2) as men age or become sick,
more testosterone is taken out of commission by binding proteins, 3) the
pituitary and hypothalamus may not release sufficient hormones to
adequately stimulate testicular testosterone production, and 4) the
testicles may have lost their ability to generate testosterone.
Testosterone also can be compromised by various
medications. For example, an elderly relative of mine was given a drug
to treat his prostate cancer. The drug works by knocking off testicular
testosterone production thereby depriving hormone-dependent cancers of
the testosterone they need to grow. Unfortunately, eliminating a key
body-strengthening hormone is not innocuous. In my relative’s case, his
six-foot, three-inch frame drastically shriveled due to osteoporosis and
muscle wasting, making me wonder, which was worse: the cancer or the
treatment.
Testosterone Replacement Therapy
Although once the realm of body-building athletes,
many have adopted TRT to mitigate the consequences of testosterone
diminution from aging or other causes. TRT-related benefits potentially
include less osteoporosis, type-2 diabetes, cardiovascular disease,
erectile dysfunction, depression and anxiety, and Alzheimer’s disease.
Although these rejuvenating benefits sound appealing, one should
approach TRT carefully, weighing the pros and cons relative to one’s
unique situation with guidance of a physician well experienced in the
issues involved.

TRT requires ongoing monitoring to manage potential
side effects. Because testosterone influences many bodily functions, it
should be prudently used. When it comes to TRT, keep in mind the old
margarine commercial: “It’s not nice to fool Mother Nature.” Modern
medicine is replete with many examples of drug-related side effects
emerging years after treatment.
A foremost consideration is that TRT should be
viewed as a long-term commitment to not only the therapy but various
medical assessments that should be carried out on an ongoing basis. TRT
will shut down testicular testosterone production. By taking
testosterone, you will disrupt the aforementioned
hypothalamic-pituitary-testicular feedback loop and turn off whatever
limited synthesis you had before treatment. As a result, if you have to
discontinue TRT for any reason, your body will be generating little
testosterone, and your physical and mental state will reflect this
paucity. The body probably will eventually recover to baseline levels,
but it may take a while.
As summarized in the table bar, TRT has used a
variety of formulations.
Potential Side
Effects
TRT should be viewed as a double-edged sword, in
which clear benefits must be balanced against potential side effects,
including the following:
Prostate Health:
Testosterone stimulates the growth of prostate cancer cells. Evidence
suggests that TRT does not cause cancer but can aggravate it if present.
With respect to the benign prostate enlargement commonly faced by many
aging men, TRT doesn’t aggravate the condition.
Blood Viscosity:
TRT stimulates red-blood-cell production, which may make the blood
overly viscous. This can compromise blood circulation, predisposing one
to high blood pressure and more strokes and heart attacks. The
condition, which occurs in a small proportion of men, can be readily
resolved by periodic blood donation.
Breast Enlargement:
If too much testosterone is converted to estrogen, men may develop
enlarged breasts. This also occurs in a small proportion of men and can
be treated with estrogen blockers.
Low Sperm: High
testosterone levels can inhibit sperm production. Men who want children
often have to discontinue TRT.
Testicular Atrophy:
Long-term TRT can cause the testicles to shrink, a reversible and
treatable condition.
Moodiness:
High-dose testosterone users (i.e., like some bodybuilders) may
experience manic episodes.
Acne and Baldness:
Because testosterone derivatives stimulate skin sebaceous gland
secretions, acne can develop. Men already losing hair may lose more
hair.
Conclusion
Part 2 will look at SCI’s disruption of
testosterone production and how that disruption may affect post-injury
health and wellness. Evidence suggests that treatment with testosterone,
an agent known to increase muscle and bone mass, may lessen functional
loss after injury.
Resource: A good starting-point reference is
Testosterone: A Man’s Guide by Nelson Vergel, available at
www.testosteronewisdom.com.
Adapted from article appearing in August 2011 Paraplegia News (For subscriptions,
call 602-224-0500) or go to
www.pn-magazine.com.
TOP