Over the years, I have noticed many friends and
colleagues with physical disabilities basking in the sun’s warmth, an
activity they can partake in as readily as any able-bodied individual.
With moderation, they should keep on basking; it’s healthy.
Although dermatologists advocate avoiding sunlight to
prevent skin damage, a growing body of science suggests that the sun
exerts many healing benefits. In fact, epidemiological studies indicate
that you are much more likely to die from disorders aggravated by chronic
underexposure to the sun than disorders aggravated by overexposure.
In just one of many examples, epidemiologists estimate at least 55 men die
prematurely from prostate cancer from too little sun for every man that
dies from too much sun.
This article’s purpose is to describe some of the
sun’s healing benefits, especially for spinal cord injury (SCI) and
multiple sclerosis (MS) and how they are mediated through vitamin-D
metabolism.
History
Throughout history, many healing modalities have
cycled in and out of favor. Sunlight (heliotherapy) was often a part of
mankind’s healing armamentaria, including that of Hippocrates, the Father
of Western Medicine. In the early twentieth century, heliotherapy was used
to treat many disorders, such as tuberculosis, rickets in children, and
war wounds. Its importance was underscored when Dr. Niels Finsen was
awarded the 1903 Nobel Prize for developing an ultraviolet (UV) treatment
for tuberculosis.
Boston’s Floating Hospital got its name because it
originally was located on a floating boat, in which children with rickets
could sunbathe. At that time, many hospitals were built to allow access to
more sunlight. Sunlight remains an important hospital-design consideration
as documented by a recent study showing that spinal-surgery patients
assigned to bright, sunny rooms needed much less pain medication.
However, as our increasingly pharmaceutically
oriented medical profession developed powerful, infection-fighting
antibiotics and drugs, and as milk and other foods were supplemented with
vitamin-D, heliotherapy faded to the background.
Its decline was greatly accelerated by the fear of
acquiring skin cancer. In my lifetime, I’ve seen a great shift on this
issue. For example, when I was a child, my mother told me to play outside
and get some sun. In contrast, today’s mothers lather sunscreen on their
children, which, in spite of good intentions, evidence suggests may
promote a vitamin-D deficiency that may have life-long implications.
Heliotherapy is once again emerging from the dark;
there is simply too much evidence supporting its use to ignore.
Ultraviolet Light
Sunlight is composed of electromagnetic radiation of
varying wavelengths, ranging from the long-wavelength infrared light to
the short-wavelength ultraviolet. The ultraviolet light is further
subdivided into UVA and the even shorter-wavelength UVB radiation.
Although UVB causes sunburns, it is also the component that initiates
Vitamin-D production in the skin.
Unfortunately, earlier sunscreens only blocked UVB,
allowing full exposure to skin-damaging UVA light. These UVB sunscreens
allowed people to absorb much more UVA radiation before becoming burned
than if no sunscreen was used at all. As such, scientists now believe that
past sunscreen use actually promoted skin damage, while, at the same time,
blocking beneficial vitamin-D production. (Sunscreen reduces the skin’s
ability to produce vitamin D by at least 95%.)
Exposure to vitamin-D-producing UVB light can vary
greatly depending upon many factors, including time of day and year; and
the latitude, altitude, and prevailing weather conditions of where we
live.
Latitude is especially important. For example, if you
live north of about 37o (roughly, a line from Richmond to San
Francisco), you will be exposed to little UVB from at least November
through February because the sun’s zenith angle is so low that the
atmosphere absorbs most UVB before it reaches you.
Because it is fat soluble, excess, sun-produced,
vitamin D is stored in body fat, and, to some degree, can be later used in
sun-deficient periods.
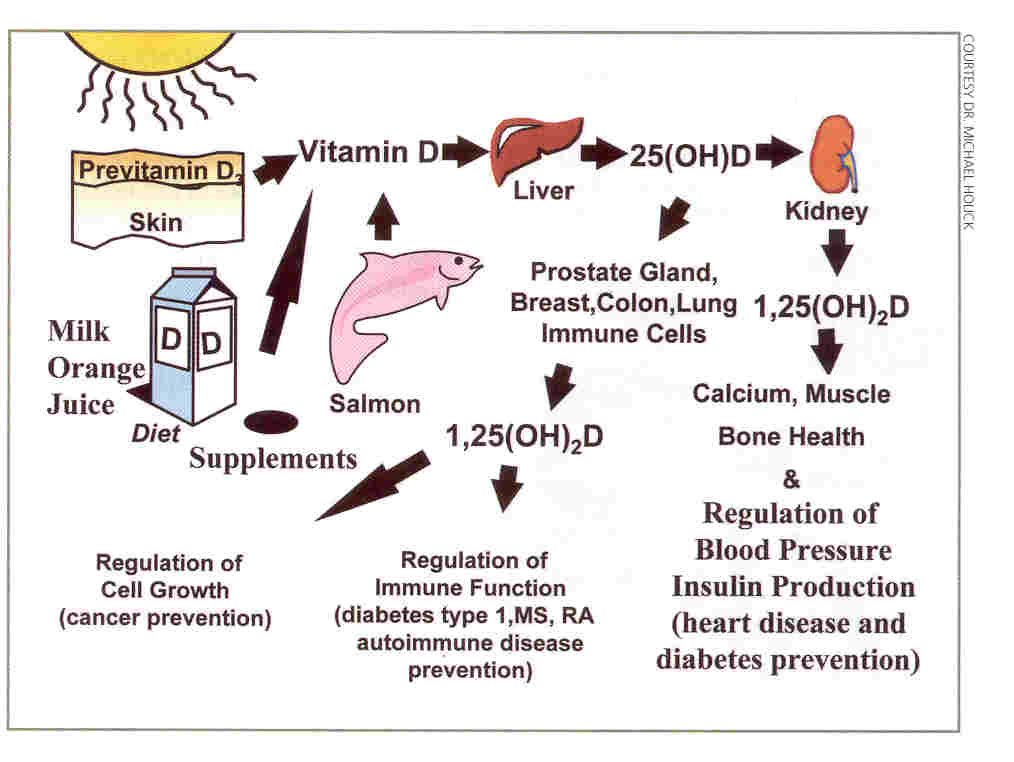
Vitamin-D Production and Metabolism
The process by which vitamin D is produced and exerts
its biological effects is complicated, involving several vitamin-D-related
molecules (see illustration).

Basically, UVB light triggers a modification of a
cholesterol-related molecule located in the membrane of skin cells. The
vitamin D that is created is then ejected from the membrane into our
circulation system, where it travels to the liver. In this organ, it is
transformed into 25-hydroxyvitamin D, the derivative that doctors use to
assess overall vitamin-D status.
The kidney, as well as some other tissues, further
converts this precursor into 1,25-hydroxyvitamin D, the most physiological
active vitamin-D metabolite, which is also called calcitrol.
Traditionally, calcitrol is understood as a hormone that, together with
parathyroid hormone, regulates blood calcium levels and, in turn, bone
density. In this role, calcitrol targets the intestine, where it promotes
calcium absorption; and bone, where it catalyzes calcium release to help
restore depleted blood calcium levels.
However, recent studies indicate that viewing
calcitrol just in this role is quite limited. In fact, the hormone exerts
a plethora of biological effects on diverse tissues, implying that this
sunlight-generated hormone sustains health throughout the body.
Although much remains to be understood, basically,
circulating calcitrol enters cells and complexes with the genes in the
cell nucleus. This affects DNA expression and, in turn, overall cell
functioning and growth. Because calcitrol maintains normal cell
proliferation, it inhibits cancerous growth. In addition, calcitrol
influences immune-cell activity, helping to explain vitamin D’s seemingly
beneficial role in infectious disease and immune-related disorders, such
as multiple sclerosis, rheumatoid arthritis, and diabetes.
Given these considerations, the implications of
preventing vitamin-D deficiency, either through sunlight or diet, are now
more profound than ever.
Vitamin-D Food Sources
Relatively few foods naturally contain vitamin D, the
most abundant being oily fish like salmon, sardines, and mackerel, or
old-fashioned, cod liver oil. Because of limited natural sources, numerous
foods, such as milk, are vitamin-D fortified.
Many scientists now believe we need 1,000 IU per day
of vitamin D (IU = international units, a measure of vitamin potency) to
avoid deficiency. For reference, a salmon serving contains about 360 IU,
a glass of fortified milk about 100 IU, an egg 25 IU, and a tablespoon of
cod liver oil 1300+ IU.
In comparison, full-body sunbathing for a period of
time that will just make you turn pink will produce 10,000-20,000 IU of
vitamin D, equivalent to 100 to 200 glasses of fortified milk. Given such
copious production, relatively casual sun exposure (arms, etc) should meet
vitamin-D needs.
Remember, however, that no vitamin D will be
generated in short-daylight months above certain latitudes. In these
periods to avoid vitamin-D deficiency - especially if you don’t like oily
fish or are lactose intolerant - you will need to consume a supplement or
use a UVB-emitting tanning bed. Studies have shown that individuals who
use such a tanning bed in winter have serum levels of 25-hydroxyvitamin D
(the marker for vitamin-D status) that is 90% higher than controls.
The importance of solar-produced vitamin D was
underscored in a study that evaluated vitamin-D status in a submarine crew
after two months of acute sun deprivation. Although the crew consumed a
vitamin-D fortified diet, their levels of this nutrient plummeted.
Vitamin D can be toxic if too much is consumed from
supplements or mistakenly over-fortified foods. However, prolonged sun
exposure does not generate toxic vitamin-D levels due to the body’s
feedback regulatory mechanisms.
At-Risk Groups
Although everyone is vulnerable to vitamin-D
deficiency, especially in winter, certain groups are particularly
predisposed. First, when exposed to the same amount of sunlight, elderly
individuals produce only 20% of the vitamin-D young adults do. As a
result, more than half of individuals older than 65 are vitamin-D
deficient.
Second, due to their skin pigmentation, African
Americans require much more sun to produce the same levels of vitamin D
than do fair-skinned Caucasians. At least 50% of African Americans, who
are also less likely to drink fortified milk due to lactose intolerance,
are vitamin-D deficient sometime during the year. Apparently, as a
consequence, they have a much greater incidence of disorders associated
with reduced sun exposure of northern latitudes.
Finally, people with spinal cord injury and multiple
sclerosis often have decreased vitamin-D levels.
SCI
As summarized in two key articles, research carried
out by Dr. William Bauman and colleagues, Bronx VA Medical Center
indicates that individuals with SCI are often vitamin-D deficient (see
Metabolism 44(12), 1995; & J Spinal Cord Med 28, 2005).
Like astronauts who lose bone density from the lack
of weight-bearing activities, paralysis causes osteoporosis. As much as
50% of lower-extremity bone mass is lost during the first several years
after injury, people with complete injuries losing the most. Hence, a
deficiency in bone-enhancing vitamin D further aggravates an already
serious SCI problem, in turn increasing fracture risk.
Bauman believes SCI predisposes one to vitamin-D
deficiency for several reasons. For example, he speculates that due to
limited mobility, someone with SCI may not get as much vitamin-D-producing
sunlight as the general population. Supporting this idea, other scientists
have demonstrated that pressure-sore-afflicted patients with SCI, who have
access to the least sunlight, have the greatest vitamin-D deficiency.
Bauman also suggests that a lack maybe be caused when
health-care professionals recommend reduced consumption of
vitamin-D-fortified dairy products under the mistaken belief that the
calcium in such foods will aggravate kidney problems. And, he believes
that many SCI-associated medicines reduce the body’s vitamin-D stores.
In his 1995 study, Bauman compared vitamin-D levels
in control subjects and in 100 veterans with SCI who averaged 20 years
post-injury. Subjects with SCI were twice as likely to have vitamin-D
levels less than that considered normal (again, the marker for vitamin-D
status in the body is 25-hydroxyvitamin D produced by the liver).
In his 2005 study, Bauman examined the effectiveness
of several dosing regimens in elevating vitamin-D levels in people with
chronic SCI. In one regimen, 40 subjects consumed 800 IU of vitamin-D per
day for 12 months. Their mean age was 43; injury duration averaged 12
years; and 17 and 23 had quadriplegia and paraplegia, respectively. Before
supplementation, 33 had below-normal vitamin-D levels; in contrast, after
12 months of supplementation, only 9 remained deficient.
Although average serum vitamin-D levels doubled in
subjects, Bauman believes that even greater supplementation is needed to
obtain nutrient serum levels needed for promoting optimal bone health in
SCI.
Multiple Sclerosis
MS is influenced by multiple interacting genetic,
environmental, nutritional, hormonal, immunological, and viral factors. It
is strongly correlated with sunlight, which is a function of latitude,
season, prevailing weather, etc. As summarized in UV Advantage by
Dr. Michael Holick (2003), MS incidence is five times greater in North
America and Europe than the tropics. In the southern US, MS prevalence is
about half that of the northern part of the country.
In one example of interacting factors, Norwegians who
live near the ocean and consume much vitamin-D-rich seafood have a lower
MS risk than those who live inland, even though both groups lack
sufficient sunlight to generate vitamin D through much of the year. In
another example, Swiss who live at lower altitudes have a greater MS risk
than those who live at high altitudes with greater exposure to
vitamin-D-producing UVB radiation.
People with MS are often vitamin-D deficient. For
example, Dr. Jeri Nieves et al. (New York) examined vitamin-D levels in 80
women with MS and determined that levels of the nutrient were often
insufficient and associated with reduced bone density. The investigators
found that dietary vitamin-D intake was less than the US Recommended Daily
Allowance (RDA) in 80% of these women, and 40% reported no sunlight
exposure, perhaps to avoid heat-aggravation of MS symptoms. In a later
study, these investigators demonstrated that over a two-year period,
fractures occurred in 22% of patients with MS compared to only 2% in age-
and gender-matched controls. Patients with MS lost bone mass at a 3-7 fold
greater rate.
Until recently, prevailing thinking was that sunlight
exerted a protective influence only early in life. Specifically, if you
got a lot of sun before age 15, your MS risk would be much less later in
life.
This thinking, however, has been challenged by Dr.
J.G. McLeod and colleagues (Australia), who examined MS prevalence in
migrants to sunny, low-latitude, low-risk Australia from cloudy,
high-latitude, high-risk United Kingdom/Ireland. Although theoretically
only those who moved before age 15 should acquire the lower Australian
MS-risk status, the investigators discovered that MS prevalence in those
who migrated before age 15 was not different than those who migrated later
in life. In other words, no matter how old you are, you may be less prone
to MS after moving to a sunnier environment.
In a suggestive pilot study, Dr. P. Goldberg et al
(Massachusetts) followed ten people with MS who consumed ~5,000 IU daily
for a year of vitamin D from cod liver oil and found that such
supplementation greatly reduced MS exacerbations. Once again, these data
suggest that protective nutritional influences are not limited to
pre-adulthood before you have ever heard of MS but may actually help when
you have it.
Recently, Harvard University investigators examined
data collected from two long-term studies involving 187,000 women. The
data indicated that those who consumed the most vitamin D had a
substantially lower MS risk than women who consumed the least amount.
Many scientists believe that vitamin D mediates its
healing influence by interacting with MS’s dysfunctional immune system.
Although this is a complex subject beyond this article’s scope, through
its hormonal metabolites, vitamin D profoundly influences the expression
of 1) a variety of immune cells, which possess gene-modulating, vitamin-D
receptors, and 2) key immune-mediating molecules called cytokines.
Vitamin D’s immune effects are supported by research
using a rodent model of MS called EAE (experimental autoimmune
encephalomyelitis). In this model, UV radiation or vitamin-D
supplementation greatly inhibited the development, severity, and duration
of EAE. In contrast, a vitamin-D deficient diet accelerated disease
progression.
Other Disorders
Evidence indicates that vitamin D prevents cancer,
diabetes, arthritis, high-blood pressure, cardiovascular disease, and
infections. In other words, it enhances overall wellness.
For example, people with SCI
are predisposed to diabetes, a disorder characterized by vitamin-D
deficiency that experimental evidence suggests reduces insulin secretion.
In another example, vitamin-D deficiency is associated with an increased
infection risk, again especially germane to infection-prone individuals
with SCI, especially in this era of antibiotic-resistant infections.
Conclusion
Whether generated through sunlight or consumed
through food or supplements, vitamin D exerts many healing benefits
relevant to individuals with spinal cord dysfunction. Given exorbitant
health-care costs, it’s nice to know that you can accrue these benefits
without paying a cent to pharmaceutical companies for costly, perhaps
side-effect-laden, drug.
Resources: Two excellent overview books are 1)
The Healing Sun by Richard Hobday (1999) and 2) The UV Advantage
by Michael Holick (2003). Much of the information in this article was
obtained from Dr. Holick’s book and his other writings.
Adapted from article appearing in June and August 2005 Paraplegia News (For subscriptions,
call 602-224-0500) or go to www.pn-magazine.com).
TOP