In its May 2003 issue, PN Magazine
was the first to report the development of a novel, function-restoring,
olfactory-tissue-transplantation procedure. Because of my involvement in
this reporting, I’ve attempted to stay abreast of developments and
periodically inform readers. This update specifically summarizes the
results of a recently published scientific study assessing the
improvements generated from using the procedure in individuals with SCI.
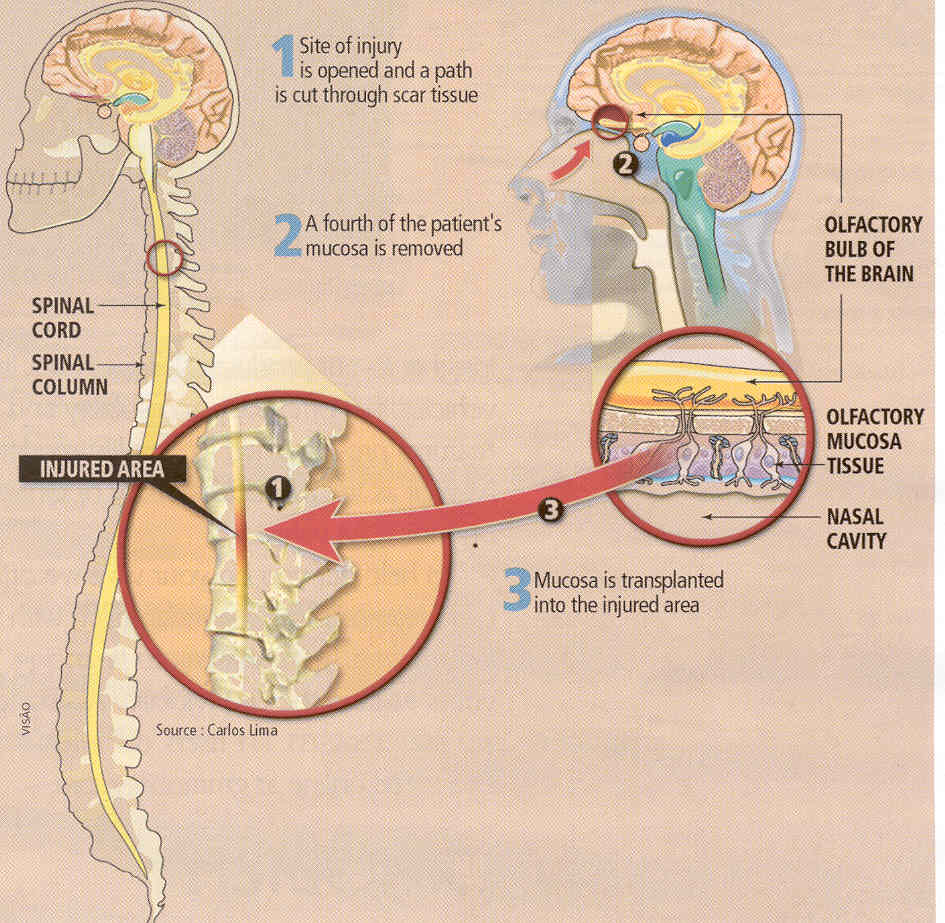
Developed by Portuguese neuropathologist Dr. Carlos
Lima and his colleagues, the procedure implants regeneratively endowed
olfactory tissue isolated from the patient’s nose into the spinal-cord
injury site. Because olfactory tissue is exposed to the air we breathe,
it contains cells with considerable turnover potential, including
renewable neurons, stem cells, and olfactory ensheathing cells (OECs).
Briefly, stem cells are progenitor cells that have the potential to
transform into a wide variety of tissue, including neuronal tissue; and
OECs promote axonal regeneration by producing insulating myelin sheaths
around axons. 
Published in a
2009 issue of the journal Neurorehabilitation and Neural Repair,
Lima’s team reported the results of transplanting olfactory tissue into
20 patients with SCI followed by extended, aggressive physical
rehabilitation. The investigators believe that three treatment
components are critical for functional improvement: 1) transplanting
stem-cell-containing olfactory-tissue (i.e., not just isolated OECs), 2)
cleaning out injury-site scar tissue to make room for transplanted
tissue and to remove regeneration barriers, and 3) intense
rehabilitation.
Patients were
required to carry out extensive physical rehabilitation both before and
after transplantation. Because there is an understandable desire to
maximize the functional benefits after any cell-transplantation
procedure, patients tend to rehabilitate much more aggressively after
transplantation than before. By so doing, it becomes difficult to
attribute any restored function to merely the transplantation. In other
words, improvement may be due to a now highly motivated individual doing
a lot of physical rehabilitation.
SUBJECTS
Ranging in age
from 19 to 37 (average 30) years, 17 men and three women were enrolled
in the study. The time lapsing from injury to transplantation varied
from 1.5 to 16 years. Because all subjects had chronic injuries,
relatively little additional recovery would be spontaneously expected,
and, as such, any improvement is most likely due to the intervention.
Injuries were sustained from traffic (14), sports (4), and work
accidents (2). Thirteen subjects had cervical injuries ranging from the
C4 to C8 level, and seven had thoracic injuries ranging from the T5 to
T12 level.
Patients were
assessed using the ASIA-impairment scale in which injuries are
classified on a scale ranging from grade A, representing a
sensory-and-motor complete injury, to grade E indicating complete
recovery. Using this scale, 15 subjects had grade A and five grade B
(motor complete) injuries at the time of transplantation. Because the
injury-site scar tissue is removed as a part of the procedure, all
lesions had to be less than three centimeters (~1.2 inches) in length
for cervical injuries and four centimeters for thoracic injuries.
PHYSICAL REHABILITATION
Subjects
averaged 32-hours per week rehabilitation for 35 weeks before
transplantation, and postoperative rehabilitation averaged 33 hours per
week for 92 weeks. Rehabilitation was undertaken at three centers, two
in Portugal and one in Italy. One center used robotic
bodyweight-supported treadmill training, and the others used an assisted
over-ground-walking training with weight bearing on the hips and feet to
promote sensory and muscle-movement feedback.
Results
indicated that the latter approach was much more effective in promoting
functional improvement after transplantation. The investigators now
believe that this method allows the freedom to promote the development
of new movement patterns that enhance functional connections.
RESULTS
Various
functional status assessments were carried out before and periodically
after transplantation. Average duration of follow-up was 28 months.
Impairment
Scales: Eleven of the 20
subjects improved one grade or more using ASIA-impairment evaluations.
Specifically, six improved from grade A complete injury to grade C
(regaining some sensation and motor function), three from grade B (motor
complete) to C, and two from grade A to B (i.e., recovery of some
sensation). Although there was considerable patient variability, on
average, motor-function, light-touch, and pin-prick scores all improved.
Walking:
Thirteen subjects from two of the three study centers were
evaluated for ambulatory improvements using the “Walking Index for
Spinal Cord Injury,” a measurement which assesses the amount of
assistance required for ambulation. All 13 demonstrated some improvement
using this evaluation, one progressing from no mobility to walking 10
meters with braces and crutches.
Functional
Independence: The same 13
subjects were also evaluated for their ability to carry out various
activities of daily living and self care (e.g., eating, grooming,
bathing, etc) by using of the FIM scale (Functional Independence
Measure). The scale is a predictor of the amount of assistance or
adaptive equipment an individual may need in everyday life. All subjects
improved their FIM scores after the transplantation-rehabilitation
intervention.
Anal:
Of the 15 subjects without anal sensation at the baseline evaluation,
nine recovered some feeling. Before the intervention, no subject was
able to do anal contraction, an ability recovered by five afterwards.
Bladder:
Of the 15 patients without bladder sensation at baseline, five regained
the ability to sense bladder fullness. One patient recovered bladder
control.
Nerve
Conduction:
Electrophysiological nerve-conduction evaluations indicated that 15
subjects could direct signals to previously paralyzed muscles.
CONCLUSION
Lima’s team
cautiously concluded that olfactory-tissue transplantation is relatively
safe and possibly beneficial in people with chronic SCI when combined
with postoperative rehabilitation. They also emphasized that neither
rehabilitation nor transplantation alone is sufficient to promote
recovery; both are needed. Furthermore, the nature of the rehabilitation
is extraordinarily important in the formation of nascent,
function-restoring, neuronal connections.
In a 2010
commentary,
Editor-in-Chief of Neurorehabilitation and Neural Repair
Dr. Bruce Dobkin (University of California, Los Angeles) notes that
Lima’s study has important implications for future SCI-focused,
cell-transplantation studies and asks the following questions:
1) “Does the type and intensity of the
rehabilitation intervention hold one of the keys to increasing the
likelihood of successful effects of cellular interventions?”
2) “Do mechanisms of
activity-dependent plasticity [i.e., neuronal adaptability] provide cell
signals that make the implants more functional?”
3) “Can a randomized clinical trial be
considered a scientifically sound comparison, unless a design like that
of Lima and colleagues is employed…?”
In recent
years, I’ve looked at numerous SCI-focused, cell-transplantation
programs emerging throughout the world. A number of them seem to produce
astonishing results in some individuals, while the results of seemingly
comparable programs are more limited. In these emerging transplantation
programs, success will be in the details, one of which is apparently the
right type of physical rehabilitation.
Adapted from article appearing in June 2010 Paraplegia News (For subscriptions,
call 602-224-0500) or go to
www.pn-magazine.com.
TOP